Trusted Nutrition Information and Support
What is Eosinophilic Esophagitis?
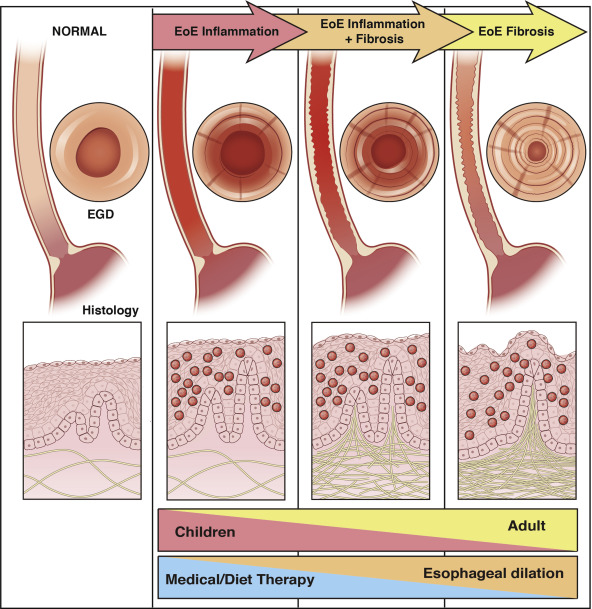
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated disease characterized by upper gastrointestinal symptoms and by pathologically increased eosinophil-predominant inflammation. Simply put, EoE is an inflammation of the tube that passes food and liquid from the mouth to the stomach caused by an overabundance of specific white blood cells.1,2
Why Does Nutrition Matter in EoE?
Get EoE resources tailored to you
Learn More Details about EoE
Symptoms of EoE may vary depending on each person and age. Children present with a broader spectrum of symptoms, including refusal of food, frequent regurgitation, vomiting, abdominal pain, reflux that does not respond to medications, painful swallowing (dysphagia), belly or chest pain, food intolerance, and poor growth.6,7
In adults, dysphagia is the most common symptom, followed by food getting stuck in the throat and reflux that does not respond to medications.6,7
In some patients with EoE -especially children-, eosinophils can build up on the stomach, small intestine, and large intestine (colon).1,2
Despite histologic remission, up to 46% of patients with EoE have persistent symptoms including dysphagia, heartburn, and chest pain. Drivers of symptoms are narrowing of the esophagus, anxiety, depression, and partial histologic remission.8
The diagnosis of EoE can only be made if it is suspected, and GI tract biopsies are obtained.9
One typical scenario in which it makes sense to investigate EoE is in patients with a lack of response to antireflux therapy, considering that an unusual presentation of gastroesophageal reflux disease is a candidate cause of EoE.10
The exact cause of EoE is unknown and likely involves multiple factors. It is suggested that EoE is caused by an immune response to specific foods and airborne allergens (proteins that trigger an immune response), leading to active inflammation and narrowing of the esophagus.11
Multiple causes can contribute to EoE, with several simultaneous “hits” required to induce the disease. Studies involving twins suggest that environmental factors play a greater role than genetics. Findings on both identical twins found that just 14.5% of the risk was attributable to genetics, with the rest determined by the twins’ surroundings. It seems that events in the prenatal environment shape the risk of EoE.12 Common chemicals, such as pesticides and food additives,13 and changes in the gut microbiome also seem to be factors making people more susceptible to EoE.14
The three main treatments for EoE are dietary management, medications, and dilation.10
Dietary Elimination
Early diet trials in children showed response rates near 100%.15 Diet elimination treatments are recognized as part of the anti-inflammatory treatment of patients with a diagnosis of EoE.9,10
Elemental diet (food allergen-free diet): comprises free amino acids, corn syrup solids, and medium-chain triglyceride oil and has been studied in both children and adults.9,16,17
- It can help achieve a histologic remission rate (drop in inflammatory cells or eosinophils in the esophagus tissue after treatment) up to 90%.
- It is associated with poor adherence and weight loss in adults.
- Often requires placement of a gastrostomy tube to bring nutrients directly to the stomach in children.
Empiric elimination diet: is defined as the removal of the six most common food allergies or removal of foods from the patient's diet based on skin prick testing and skin patch testing.
- 6 food elimination diet (SFED): it is the most studied and removes milk, wheat, soy, egg, nuts/peanuts, and fish/shellfish.
- 4-food elimination diet (FFED): it removes dairy, gluten-containing cereals, egg, and legumes.21,22
- Overall efficacy rates between 54% (adults) and 65% (children).
- 2-food elimination diet (TFED): it removes dairy and gluten-containing cereals and has been studied in children and adults.23
- Overall efficacy rates between 40% (adults) and 44% (children).
- Reduced the number of endoscopies by 20%.
- Milk-only elimination diet (1FED): it removes all animal milk.24
- Overall efficacy of 51% (children).
- It is easy to implement and follow.
- Serum IgE-targeted elimination diets: elimination diets based on skin or serum antibody test results have limited success in predicting foods that trigger EoE.10 ,25
- Emerging evidence has questioned the involvement of IgE in the onset and development of EoE.
- No longer recommended to guide the diet therapy of EoE.
Either a step-up or step-down approach is very reasonable based on the goals and motivation of the patient.26


The latest guidelines support recommending less-restrictive diets as a primary treatment based on patient preferences.10, 26
Providers may consider starting with a less-restrictive empiric diet (e.g., 1FED or 2FED) as first-line treatment before moving towards more-restrictive diets (e.g., 6FED).
Challenges in the dietary management of EoE are:
- Food reintroduction after the removal of suspected or known food triggers
- Trigger identification
Drugs
- Biologics
- Topical corticosteroids: budesonide
- Acid suppressors (proton pump inhibitors)
- Small molecules (under study)
Dilation
Esophageal dilation should be used in parallel with anti-inflammatory therapy in patients with esophageal strictures and dysphagia.
Symptoms of EoE may vary depending on each person and age. Children present with a broader spectrum of symptoms, including refusal of food, frequent regurgitation, vomiting, abdominal pain, reflux that does not respond to medications, painful swallowing (dysphagia), belly or chest pain, food intolerance, and poor growth.6,7
In adults, dysphagia is the most common symptom, followed by food getting stuck in the throat and reflux that does not respond to medications.6,7
In some patients with EoE -especially children-, eosinophils can build up on the stomach, small intestine, and large intestine (colon).1,2
Despite histologic remission, up to 46% of patients with EoE have persistent symptoms including dysphagia, heartburn, and chest pain. Drivers of symptoms are narrowing of the esophagus, anxiety, depression, and partial histologic remission.8
The diagnosis of EoE can only be made if it is suspected, and GI tract biopsies are obtained.9
One typical scenario in which it makes sense to investigate EoE is in patients with a lack of response to antireflux therapy, considering that an unusual presentation of gastroesophageal reflux disease is a candidate cause of EoE.10
The exact cause of EoE is unknown and likely involves multiple factors. It is suggested that EoE is caused by an immune response to specific foods and airborne allergens (proteins that trigger an immune response), leading to active inflammation and narrowing of the esophagus.11
Multiple causes can contribute to EoE, with several simultaneous “hits” required to induce the disease. Studies involving twins suggest that environmental factors play a greater role than genetics. Findings on both identical twins found that just 14.5% of the risk was attributable to genetics, with the rest determined by the twins’ surroundings. It seems that events in the prenatal environment shape the risk of EoE.12 Common chemicals, such as pesticides and food additives,13 and changes in the gut microbiome also seem to be factors making people more susceptible to EoE.14
The three main treatments for EoE are dietary management, medications, and dilation.10
Dietary Elimination
Early diet trials in children showed response rates near 100%.15 Diet elimination treatments are recognized as part of the anti-inflammatory treatment of patients with a diagnosis of EoE.9,10
Elemental diet (food allergen-free diet): comprises free amino acids, corn syrup solids, and medium-chain triglyceride oil and has been studied in both children and adults.9,16,17
- It can help achieve a histologic remission rate (drop in inflammatory cells or eosinophils in the esophagus tissue after treatment) up to 90%.
- It is associated with poor adherence and weight loss in adults.
- Often requires placement of a gastrostomy tube to bring nutrients directly to the stomach in children.
Empiric elimination diet: is defined as the removal of the six most common food allergies or removal of foods from the patient's diet.
- Milk-only elimination diet (1FED): it removes all animal milk.24
- Overall efficacy of 51% (children).
- It is easy to implement and follow.
- 2-food elimination diet (TFED): it removes dairy and gluten-containing cereals and has been studied in children and adults.23
- Overall efficacy rates between 40% (adults) and 44% (children).
- Reduced the number of endoscopies by 20%.
- 4-food elimination diet (FFED): it removes dairy, gluten-containing cereals, egg, and soy.21,22
- Overall efficacy rates between 54% (adults) and 65% (children).
- 6 food elimination diet (SFED): it is the most studied and removes milk, wheat, soy, egg, nuts/peanuts, and fish/shellfish.
Serum IgE-targeted elimination diets: elimination diets based on skin or serum antibody test results have limited success in predicting foods that trigger EoE.10 ,25
- Emerging evidence has questioned the involvement of IgE in the onset and development of EoE.
- No longer recommended to guide the diet therapy of EoE.
Either a step-up or step-down approach is very reasonable based on the goals and motivation of the patient.26
The latest guidelines support recommending less-restrictive diets as a primary treatment based on patient preferences.10, 26
Providers may consider starting with a less-restrictive empiric diet (e.g., 1FED or 2FED) as first-line treatment before moving towards more-restrictive diets (e.g., 6FED).
Challenges in the dietary management of EoE are:
- Food reintroduction after the removal of suspected or known food triggers
- Trigger identification
Drugs
- Biologics
- Topical corticosteroids: budesonide
- Acid suppressors (proton pump inhibitors)
- Small molecules (under study)
Dilation
Esophageal dilation should be used in parallel with anti-inflammatory therapy in patients with esophageal strictures and dysphagia.
Delicious and Nutritious Recipes

.svg)





%20%26%20Spinach%20Curry.jpg)

Search Our Resource and Lifestyle Database


Gain Knowledge with Our Research
References
- Liacouras LA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults. JACI. 2011; 128(1):3-20.e6; quiz 21-2. doi: 10.1016/j.jaci.2011.02.040.
- Dellon ES, Gonsalves N, Abonia JP, et al. International consensus recommendations for eosinophilic gastrointestinal disease nomenclature. CGH. 2022; 20(11):2474-2484.e3. doi: 10.1016/j.cgh.2022.02.017.
- Dellon ES, Hirano I. Epidemiology and natural history of eosinophilic esophagitis. Gastroenterology. 2017; 154(2):319–332.e3. doi: 10.1053/j.gastro.2017.06.067.
- Visaggi P, Dellon ES. Epidemiology, natural history, and treatment of eosinophilic gastrointestinal diseases. Gastroenterology. 2025. doi: 10.1053/j.gastro.2025.09.030. Article in press.
- Mona R, Hruz P. Epidemiology of Eosinophilic Esophagitis: Really a Novel and Evolving Disease? Inflamm Intest Dis. 2025 Jan 20;10(1):34-40. doi: 10.1159/000543022. PMID: 39834520; PMCID: PMC11745509.
- AGA GI patient center. Eosinophilic esophagitis. AGA. Available: https://patient.gastro.org/eosinophilic-esophagitis/
- Laserna-Mendieta EJ, Navarro P, Casabona-Francés S, et al. Differences between childhood- and adulthood-onset eosinophilic esophagitis: An analysis from the EoE connect registry. Dig Liver Dis. 2023; 55(3):350-359. doi: 10.1016/j.dld.2022.09.020.
- Beveridge CA, Hermanns C, Thanawala S, et al. Predictors of persistent symptoms in eosinophilic esophagitis after remission: fibrostenosis, eosinophilia, anxiety, and depression. Dis Esophagus. 2025; 38(1):doae110. doi: 10.1093/dote/doae110.
- Kelly KJ, Lazenby AJ, Rowe PC, et al. Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology. 1995; 109(5):1503-12. doi: 10.1016/0016-5085(95)90637-1.
- Dellon ES, Muir AB, Katzka DA, et al. ACG clinical guideline: diagnosis and management of eosinophilic esophagitis. Am J Gastroenterol. 2025; 120(1):31-59. doi: 10.14309/ajg.0000000000003194.
- Young E, Philpott H. Pathophysiology of dysphagia in eosinophilic esophagitis: causes, consequences, and management. Dig Dis Sci. 2022; 67(4):1101-1115. doi: 10.1007/s10620-022-07419-6.
- Alexander ES, Martin LJ, Collins MH, et al. Twin and family studies reveal strong environmental and weaker genetic cues explaining heritability of eosinophilic esophagitis. J Allergy Clin Immunol. 2014; 134(5):1084-1092.e1. doi: 10.1016/j.jaci.2014.07.021.
- Doyle AD, Masuda MY, Pyon GC, et al. Detergent exposure induces epithelial barrier dysfunction and eosinophilic inflammation in the esophagus. Allergy. 2023; 78(1):192-201. doi: 10.1111/all.15457.
- Jensen ET, Kuhl JT, Martin LJ, et al. Early-life environmental exposures interact with genetic susceptibility variants in pediatric patients eith eosinophilic esophagitis. J Allergy Clin Immunol. 2018; 141(2):632-637.e5. doi: 10.1016/j.jaci.2017.07.010.
- Bohm M, Richter JE. Treatment of eosinophilic esophagitis: overview, current limitations, and future direction. Am J Gastroenterol. 2008; 103(10):2635-44; quiz 2645. doi: 10.1111/j.1572-0241.2008.02116.x.
- Peterson KA, Byrne KR, Vinson LA, et al. Elemental diet induces histologic response in adult eosinophilic esophagitis. Am J Gastroenterol. 2013; 108(5):759-66. doi: 10.1038/ajg.2012.468.
- Arias A, González-Cervera J, Tenias JM, et al. Efficacy of dietary interventions for inducing histologic remission in patients with eosinophilic esophagitis: a systematic review and meta-analysis. Am J Gastroenterol. 2014; 146(7):1639-48. doi: 10.1053/j.gastro.2014.02.006.
- Kagalwalla AF, Sentongo TA, Ritz S, et al. Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2006; 4(9):1097-102. doi: 10.1016/j.cgh.2006.05.026.
- Gonsalves N, Yang GY, Doerfler B, et al. Elimination diet effectively treats eosinophilic esophagitis in adults; food reintroduction identifies causative factors. Gastroenterology. 2012; 142(7):1451-1459. doi: 10.1053/j.gastro.2012.03.001.
- Lucendo AJ, Arias A, González-Cervera J, et al. Empiric 6-food elimination diet induced and maintained prolonged remission in patients with adult eosinophilic esophagitis: a prospective study on the food cause of the disease. JACI. 2013; 131(3):797-804. doi: 10.1016/j.jaci.2012.12.664.
- Molina-Infante J, Arias A, Barrio J, et al. Four-food group elimination diet for adult eosinophilic esophagitis: A prospective multicenter study. JACI. 2014; 134(5):1093-9.e1. doi: 10.1016/j.jaci.2014.07.023.
- Kagalwalla AF, Wechsler JB, Amsden K, et al. Efficacy of a 4-food elimination diet for children with eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2017; 5(11):1698-1707.e7. doi: 10.1016/j.cgh.2017.05.048.
- Molina-Infante J, Lucendo AJ. Dietary therapy for eosinophilic esophagitis. JACI. 2018; 142(1):41-47. doi: 10.1016/j.jaci.2018.02.028.
- Wechsler JB, Schwartz S, Arva NC, et al. A single-food milk elimination diet is effective for treatment of eosinophilic esophagitis in children. Clin Gastroenterol Hepatol. 2022; 20(8):1748-1756.e11. doi: 10.1016/j.cgh.2021.03.049.
- Mayerhofer C, Kavallar AM, Aldrian D, et al. Efficacy of elimination diets in eosinophilic esophagitis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2023; 21(9):2197-2210.e3. doi: 10.1016/j.cgh.2023.01.019.
- Visaggi P, Baiano Svizzero F, Savarino E. Food elimination diets in eosinophilic esophagitis: Practical tips in current management and future directions. Best Pract Res Clin Gastroenterol. 2023; 62-63:101825. doi: 10.1016/j.bpg.2023.101825.
