
Copied
ECCO’26: A Leap Forward in Integrating Nutrition in IBD Care, But Still Some Areas of Debate
Discover what’s new and interesting about the role of nutrition and diet in the management of IBD based on etiology.
In February 2026, the GI Nutrition Foundation attended the 21st Congress of ECCO (ECCO’26) in Stockholm, Sweden. With more than 7,300 attendees from 98 countries, this year's congress theme focused on ‘holistic IBD care’. The scientific programme covered emerging treatments in IBD, with particular interest in dietary and nutrition-based approaches, increasingly recognized as integral to multidisciplinary IBD management.
Access to IBD diagnostic tools and therapies is unequal
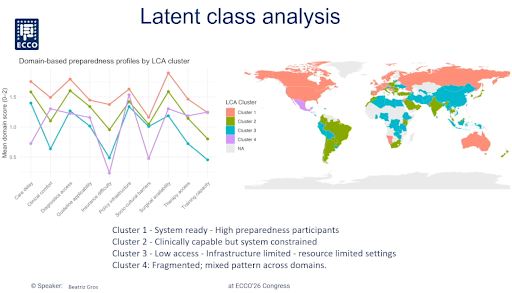
On behalf of the new Lancet Global Commission on IBD, Beatriz Gros, PhD, MD, from Reina Sofía University Hospital of Córdoba (Spain), acknowledged that marked disparities in IBD care persist worldwide despite therapeutic advances. The countries in the Global South are characterized by:
- Patients have less access to multidisciplinary teams and to standard-of-care tests (fecal calprotectin and imaging techniques)
- Unequal access to all treatments (not just advanced, even biosimilars), due to cost, insurance, and availability issues, while patients are less reluctant to start drugs
- Healthcare providers (including dietitians) have fewer training opportunities, while those in the countries in the Global North have less time for training
Shaji Sebastian, MD, PhD, from Hull University Teaching Hospitals (United Kingdom), acknowledged that newly industrialized countries (e.g., Brazil) are seeing an acceleration in the new cases of IBD, which mirrors its progression in the Western world during the 20th century1. Some strategies to improve global IBD care by bridging high-income and low- and middle-income countries include decentralization and diagnostic innovation, standardized global education, sustainable access to advanced IBD treatments, and equitable research partnerships. In alignment with the World Health Organization package of essential noncommunicable principles, to meet the upcoming challenges in IBD care, there is a need to move from specialized urban centers to the community level and to focus on long-term stability and prevention rather than acute flare management2.
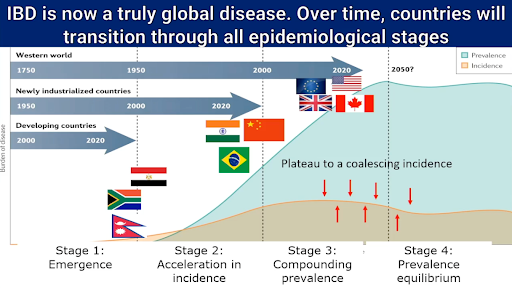
“The most important question for each of us in the IBD community is “How did we transition from a handful of cases in the West a century ago to millions of patients globally today and how will we prepare for this epidemic of IBD?”.
Shaji Sebastian, MD, PhD, IBD Service Lead at Hull University Teaching Hospitals (UK)
IBD starts before diagnosis
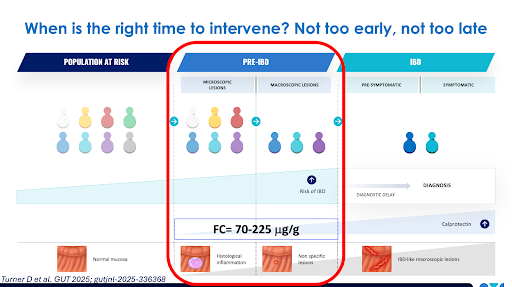
The rising ubiquity of IBD needs the development of prevention strategies for at-risk individuals. Dan Turner, MD, PhD, from the Hebrew University of Jerusalem (Israel), presented results from the PIONIR trial (Preventing IBD ONset in Individuals at Risk), which explored whether the Tasty&Healthy diet, based on whole foods and without formulas, could improve markers of inflammation in first-degree relatives of patients with Crohn’s disease (CD) who were at high risk of developing Crohn’s.
Of 331 healthy first-degree relatives with elevated fecal calprotectin levels (>70 mcg/g in two or more tests), 29 eligible individuals without Crohn’s-related mucosal changes (deemed to be in a potential pre-Crohn’s disease stage) were randomnly assigned to either the Tasty&Healthy diet or to continue their habitual diet for 8 weeks, followed by crossover to alternate diet for a further 8 weeks. The analysis of both treatment phases showed that there was a 38% decrease from baseline in fecal calprotectin with the habitual diet (likely reflecting the placebo effect), while there was a 61% decrease with the Tasty&Healthy diet (37% of reduction of fecal calprotectin with the Tasty & Healthy diet compared to the habitual diet; ratio 0.63, 95% CI 0.51-0.80; p<0.001). The T&H diet was easily followed by up to 86% of participants, and Turner acknowledged that, after finishing the trial, most participants continued following the diet, which is personalized for each family under the guidance of a dietitian.
“Nutritional interventions may treat the cause of IBD rather than “early treatment” with anti-inflammatory drugs, which have adverse events and are costly”.
Dan Turner, MD, PhD, professor of Paediatrics at the Hebrew University of Jerusalem (Israel)
The best of combining biologics and diet therapies for better management of Crohn’s disease
A workshop sponsored by Nestlé Health Science addressed the latest evidence, clinical experience, and practical strategies for combining drugs and diet to optimize outcomes for patients with CD. Prof. Eytan Wine, MD, PhD, FRCPC, from Hospital for Sick Children and University of Toronto, introduced the session by highlighting that the upcoming ECCO-ESPGHAN guidelines on the medical management of pediatric CD recognize the use of both an only-liquid diet and Crohn’s Disease Exclusion Diet options as an induction therapy in children with CD.
Prof. Kostas Gerasimidis, RD, PhD, from the University of Glasgow (UK), shared lessons from the BIOPIC Study (BIOlogics and Partial enteral nutrition In Crohn’s Disease) investigating whether replacing of 50% of habitual food intake with specialized milkshakes improves remission rates and remission maintenance in adults with active CD treated with first-line adalimumab.
Gerasimidis showed that the combination of biologics and partial enteral nutrition (involving the replacement of 50% of a person’s habitual diet with oral formula, while allowing the flexibility of incorporating regular table foods) yielded better responses in patients who were “sicker” (high baseline C-reactive protein and fecal calprotectin) and in whom the ileum was involved. These benefits were accompanied by higher rates of endoscopic response and might be partly explained by increases in 13 specific immune cell populations in the blood, with most cells returning to normal levels seen in healthy people. It is also worth noting that the combined treatment was associated with improvements in the micronutrient profile and with high muscle mass and grip strength (a non-invasive marker of muscle function, nutritional status, and frailty).
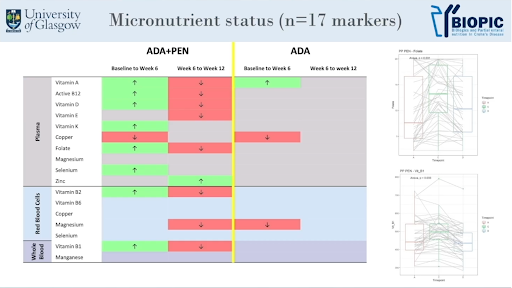
“Combining biologics and diet therapies can be seen as a 'two-in-one treatment' that improves disease activity and nutritional parameters”.
Kostas Gerasimidis, RD, PhD, professor of clinical nutrition at the University of Glasgow (UK)
Luca Scarallo, MD, PhD, from Meyer Children’s Hospital IRCCS (Italy), presented data on patients with IBD collected from various centres, showing that combining the Crohn’s Disease Exclusion Diet (CDED) with partial enteral nutrition and biologics may enhance biologic efficacy and reduce unnecessary therapeutic escalation targeting initial disease roots (e.g., a disrupted gut barrier and gut microbiota) that trigger inflammation much before symptoms appear.
Rotem Sigall Boneh, RD, PhD, from Wolfson Medical Center (Israel), addressed challenges and opportunities for combined diet and medical therapy. While biologics are highly effective, not all patients achieve remission, a loss of response is common, and long-term maintenance remains challenging. The CDED plus nutritionally complete formulas are an effective therapy now integrated into CD guidelines and applications include using it as a bridge therapy option before biologics5, as a rescue therapy in patients who lost response to biologics6, to reduce subclinical inflammation in asymptomatic pediatric patients with CD7, and to enhance biologic effectiveness8. Sigall Boneh is now working on the DISPENSE-T Study, which explores whether adding a modified CDED to infliximab improves clinical and biochemical responses in children with CD.
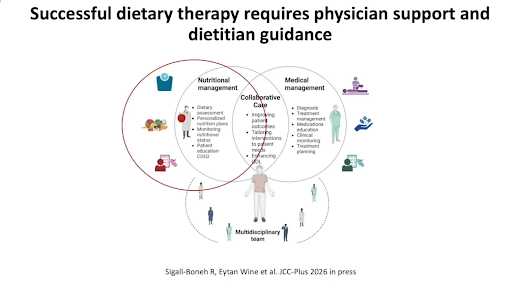
“Combined dietary and biologic therapy is a marathon, not a sprint, and offers a complementary, mechanism-based approach in patients who do not achieve sustained remission”.
Rotem Sigall Boneh, RD, PhD, E. Wolfson Medical Center (Israel)
Dietary advice in ulcerative colitis: what’s new?
The best diet for ulcerative colitis (UC) is currently unknown. Alice Day, RD, PhD, from the Queen Elizabeth Hospital (Australia), updated the knowns and unknowns on the role of whole-food diets in igniting or extinguishing inflammation in UC. Recent findings from the PREdiCCt trial in patients with UC in remission revealed that higher habitual total meat intake is associated with a double risk of an objective flare, with the strongest signals for unprocessed red and white meat, while fish is not associated with flare risk9. In contrast, fiber from fruits and vegetables may be protective against the development of UC10, while fiber supplements are not enough to correct the altered gut microbiome in UC11. A Mediterranean diet pattern is associated with the maintenance of clinical remission and reduced fecal calprotectin in patients with inactive UC through favouring protective gut bacteria and increasing short-chain fatty acids while downloading pro-inflammatory metabolites12,13.
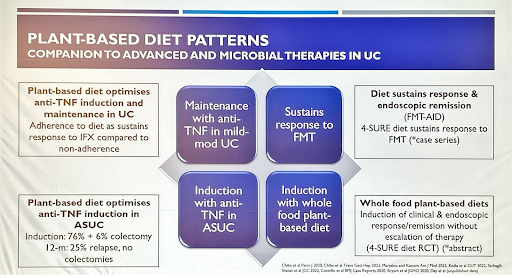
The manipulation of the balance between dietary fiber and protein in favor of fiber in the form of whole foods could affect bowel function and clinical disease activity scores in UC14. Based on this hypothesis, the Four Strategies to SUlphide Reduction (4-SURE) diet acts by reducing harmful sulfide production in the gut and is based on the rationale that UC is confined to the large bowel, which is the primary site for gut microbiota fermentation of fiber and protein. It has the potential of inducing clinical response/remission, early mucosal healing, regression of inflammation, and histological response15.
Another diet of potential interest for patients with UC is the novel UC-TREAT diet, designed to reduce gut inflammation by modifying the gut microbiome. It is rich in fermentable fiber (providing 35 g/day fiber in addition to habitual intake) and includes 5 daily fermented foods plus 2 portions/day of berries and a multivitamin supplement. A small controlled prospective trial showed that the UC-TREAT diet is acceptable and tolerable to adults with UC in remission and does not alter the disease state16.
Unresolved questions in dietary management of UC are whether patients with UC can ferment fiber, can benefit from higher fiber intake, the most appropriate source, amount, and type of fiber, and macro- and micronutrient requirements in quiescent and mild-moderate disease17.
Gut-brain axis in IBD
The ECCO lecture was given by Qasim Aziz, MD, PhD, from Queen Mary University of London (UK), on the ‘Gut-brain axis in IBD’. Almost a fourth of patients with IBD, whether in remission or in the active state, have features of irritable bowel syndrome. In the remission state, IBS seems to be more common in CD than it is in UC18. These findings show that persistent symptoms remain even in patients with IBD in remission, reflecting IBD is not just mucosal inflammation and it is also a gut-brain axis dysregulation involving a lower tolerance of pain, immune activation and psychological distress being more common in patients with IBD featuring IBS-like symptoms compared with patients without IBS.
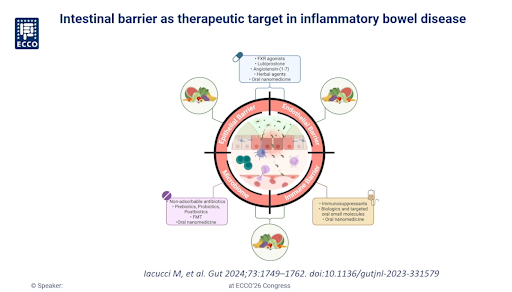
Dietary interventions such as probiotics, prebiotics and postbiotics may likely offer a benefit for patients with IBD by reducing the inflammation in the gut epithelium and reinforcing gut integrity19. This translates into potential benefits of probiotics, prebiotics, and synbiotics in inducing IBD remission and improving UC activity, but not in preventing IBD recurrence or improving CD disease activity20.
“IBD is not just mucosal inflammation. Future IBD care must target the gut barrier, microbiome, nervous system and brain, not just the bowel”.
Qasim Aziz, MD, PhD, Queen Mary University of London (UK)
Britta Siegmund, MD, PhD, from Charité-Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin (Germany), updated the role of immune system ageing and the intestinal barrier in older patients with IBD. Gut inflammation markers (zonulin and calprotectin) show age-dependent variation in adult patients with UC, with low endogenous vitamin D levels associated with high zonulin levels, suggesting a protective role of vitamin D against gut inflammation. According to Siegmund, resetting immunosenescence in older IBD emerges as a potential therapeutic target in this population21.
The 22nd Congress of ECCO will take place 3-6 March 2027 in Copenhagen, Denmark.

References:
- Hracs L, Windsor JW, Gorospe J, et al. Global evolution of inflammatory bowel disease across epidemiologic stages. Nature. 2025;642(8067):458-466. doi: 10.1038/s41586-025-08940-0.
- Singh A, Bhardwaj A, Jena A, et al. Patient knowledge and awareness on inflammatory bowel disease as it evolves as a global disease: a scoping review. J Crohns Colitis. 2026; 20(3):jjag019. doi: 10.1093/ecco-jcc/jjag019.
- Turner D, Kenigsberg S, Focht G, et al. Preclinical stages of Crohn’s disease defined by faecal calprotectin in asymptomatic first-degree relatives: screening framework for prevention trials. Gut. First published online 2025. doi: 10.1136/gutjnl-2025-336368.
- Aharoni-Frutkoff Y, Plotkin L, Pollak D, et al. Whole food diet induces remission in children and young adults with mild to moderate Crohn’s disease and is more tolerable than exclusive enteral nutrition: a randomized trial. Gastroenterology. 2025; 169(7):1462-1474.e2. doi: 10.1053/j.gastro.2025.06.011.
- Sigall Boneh R, Van Limbergen J, Wine E, et al. Dietary therapies induce rapid response and remission in pediatric patients with active Crohn’s disease. Clin Gastroenterol Hepatol. 2021; 19(4):752-759. doi: 10.1016/j.cgh.2020.04.006.
- Sigall Boneh R, Sarbagili Shabat C, Yanai H, et al. Dietary therapy with the Crohn’s Disease Exclusion Diet is a successful strategy for induction of remission in children and adults failing biological therapy. J Crohns Colitis. 2017; 11(10):1205-1212. doi: 10.1093/ecco-jcc/jjx071.
- Soledad Arcucci M, Menendez L, Orsi M, et al. Role of adjuvant Crohn’s disease exclusion diet plus enteral nutrition in asymptomatic pediatric Crohn’s disease having biochemical activity: A randomized, pilot study. Indian J Gastroenterol. 2024; 43(1):199-207. doi: 10.1007/s12664-023-01416-x.
- Pochesci S, Scarallo L, Miraglia T, et al. Crohn’s disease exclusion diet as an add-on to antitumor necrosis factor-α therapy in children with moderate-to-severe Crohn’s disease. J Pediatr Gastroenterol Nutr. 2025; 81(5):1237-1241. doi: 10.1002/jpn3.70208.
- Constantine-Cooke N, Gros B, Plevris N, et al. Associations between demographic, clinical and dietary factors and flares in inflammatory bowel disease: the PRognostic effect of Environmental factors in Crohn’s and Colitis (PREdiCCt) prospective cohort study. Gut. 2026. doi: 10.1136/gutjnl-2025-337846.
- Milajerdi A, Ebrahimi-Daryani N, Dieleman LA, et al. Association of dietary fiber, fruit, and vegetable consumption with risk of inflammatory bowel disease: a systematic review and meta-analysis. Adv Nutr. 2020;12(3):735–743. doi: 10.1093/advances/nmaa145.
- Gerasimidis K, Nichols B, McGowan M, et al. The effects of commonly consumed dietary fibres on the gut microbiome and its fibre fermentative capacity in adults with inflammatory bowel disease in remission. Nutrients. 2022;14(5):1053. doi: 10.3390/nu14051053.
- Haskey N, Estaki M, Ye J, et al. A Mediterranean diet pattern improves intestinal inflammation concoimitant with reshaping of the bacteriome in ulcerative colitis: a randomised controlled trial. J Crohns Colitis. 2023;17(10):1569-1578. doi: 10.1093/ecco-jcc/jjad073.
- Haskey N, Ye J, Josephson J, et al. Metabolomic signatures highlight fiber-degrading Bacteroides species in Mediterranean diet response among ulcerative colitis. Gastro Hep Adv. 2024; 4(4):100606. doi: 10.1016/j.gastha.2024.100606.
- Davis RH, Bryant RV, Gibson PR, et al. The fate of dietary protein in the gastrointestinal tract and implications for colonic disease. Nat Rev Gastroenterol Hepatol. 2026. doi: 10.1038/s41575-026-01173-0.
- Day A, Portmann L, Goodsall T, et al. A randomised placebo-controlled dietary advice trial of the Four Strategies to SUlphide Reduction (4-SURE) diet in adults with mild-moderately active ulcerative colitis. J Crohns Colitis. 2026; 20(Suppl. 1):jjaf231.1312. doi: 10.1093/ecco-jcc/jjaf231.1312.
- Mckirdy S, Gaya D, Russell RK, et al. Impact of the novel UC-TREAT diet on the gut microbiome and its tolerability in healthy adults and adults with quiescent ulcerative colitis. J Crohns Colitis. 2026; 20(Suppl. 1):jjaf231.776. doi: 10.1093/ecco-jcc/jjaf231.776.
- Plush S, Bryant RV, Davis RH, et al. Nutrient requirements for adults with ulcerative colitis over the disease course: a systematic scoping review. Crit Rev Food Sci Nutr. 2026; 1-12. doi: 10.1080/10408398.2026.2620433.
- Halpin SJ, Ford AC. Prevalence of symptoms meeting criteria for irritable bowel syndrome in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2012; 107(10):1474-82. doi: 10.1038/ajg.2012.260.
- Iacucci M, Santacroce G, Majumder S, et al. Opening the doors of precision medicine: novel tools to assess intestinal barrier in inflammatory bowel disease and colitis-associated neoplasia. Gut. 2024; 73(10):1749-1762. doi: 10.1136/gutjnl-2023-331579.
- Zhang XF, Guan XX, Tang YJ, et al. Clinical effects and gut microbiota changes of using probiotics, prebiotics or synbiotics in inflammatory bowel disease: a systematic review and meta-analysis. Eur J Nutr. 2021; 60(5):2855-2875. doi: 10.1007/s00394-021-02503-5.
Merino JJ, Bastande Rey M, Fernández-García R. Microbiota and gut inflammatory markers (zonulin and fecal calprotectin) exhibit age-dependent variation in patients with ulcerative colitis. Nutrients. 2025; 15(9):1412. doi: 10.3390/life15091412.

Andreu Prados is a science and medical writer specializing in making reliable evidence of non-prescription therapeutics for gastrointestinal conditions understandable, engaging and ready for use for healthcare professionals and patients.




Support our Mission
Your donation will help us to enhance the well-being and health outcomes of patients with GI conditions.
Donate