
Copied
DDW 2026: Key Takeaways on Nutrition and Diet in GI Disorders
From 2 to 5 May 2026, GI Nutrition Foundation attended Digestive Disease Week® in Chicago, USA, with more than 14,260 attendees (in person and online). Learn more about what’s new and interesting in nutrition care for IBS, IBD, celiac disease, and eosinophilic esophagitis.

Nutritional Tips and Tricks in Challenging GI Conditions
IBS and related conditions are diagnoses we can actively understand and treat, rather than diagnoses of exclusion. Nutrition care for IBS is shifting from restricted diets to personalized, patient-centered interventions, but the challenge is applying good science thoughtfully, whether that’s looking at diet, the gut microbiome, or increased sensitivity to pain, to improve patient outcomes. Immune activation, rather than classical IgE-mediated food allergy, is an emerging factor involved in disorders of gut-brain interaction (DGBI). Jan Tack, MD, PhD, from the University of Leuven, acknowledged that existing studies have methodological limitations, particularly in the selection of a relevant sham arm, so food allergy and intolerance tests are not ready for routine clinical use. Eamonn M. Quigley, MD, PhD, chief of Gastroenterology at the Houston Methodist Hospital, acknowledged that food influences almost all causes of disorders of gut-brain interaction and guidance from a specialized dietitian is key, as the interpretation of studies is often complicated by methodological shortcomings1.

Up to 50% with patients with DGBI have reduced appetite, which complicates the symptoms and long-term care2. Among IBD patients, appetite was significantly reduced both before and after eating, and is thought to be driven in part by elevated early satiety hormones such as PYY and ghrelin that were found to revert to normal levels when in disease remission3. Kimberly Harer, MD, ScM, from the University of Michigan, shared that the first step is to talk to the patient and ask follow-up questions (i.e., “toddler interrogation”) to dig deep to understand what the patient is experiencing and work to identify the disruptive mechanisms. Next up, we want to identify potential contributors and ask whether any new medications were started around the time the change in appetite appeared. We then want to assess their dietary patterns. The final two steps are to help risk-stratify the patient. We want to assess their weight trend (not just BMI, as not all malnourished patients have low BMI) and any red-flag symptoms that would require further evaluation and targeted testing. Treating low appetite includes dietary strategies and pharmacologic treatment options and should involve the patient, gastroenterologist, dietitian, and a psychologist specializing in GI behavioral health.
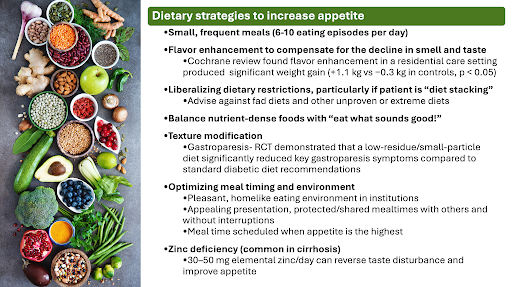
It is also important to highlight that diet is not always the only solution. Not all patients are good candidates for dietary approaches, and the GI provider should get comfortable with a quick-and-dirty dietary recall, challenge maladaptive beliefs while respecting the patient's experience, and provide alternative explanations for patients’ symptoms. This is particularly relevant for patients with bloating, in whom diaphragmatic contraction and relaxation of the abdominal wall, rather than excessive gas in the abdomen, is the most likely cause of a pregnant-like abdomen4. Another research involving a large UK cohort of more than 1.2 million primary care patients found a strong association between IBS and infertility. Researchers also identified a smaller but still significant association between infertility and functional dyspepsia, whereas chronic constipation was not associated with infertility. As an increased rate of infertility is associated with endometriosis and celiac disease (both considered “IBS mimickers”), when infertility is present along with an IBS diagnosis, screening for endometriosis and celiac disease should be considered5.

Dietary and Psychosocial Care Matter in Newly Diagnosed IBD
A clinical session explored the impact of early treatment on the natural history of IBD and highlighted that proactive care of IBD involves both identifying patients before they have severe disease and identifying patients at risk for severe disease. Dietary and psychosocial support were featured as important as the medications in newly diagnosed IBD. Iris Dotan, MD, PhD, Director of the Division of Gastroenterology at the Rabin Medical Center (Israel), acknowledged that guidelines endorse both dietary and psychosocial care, which complement remission-related biomarkers for optimal IBD management from diagnosis onward.
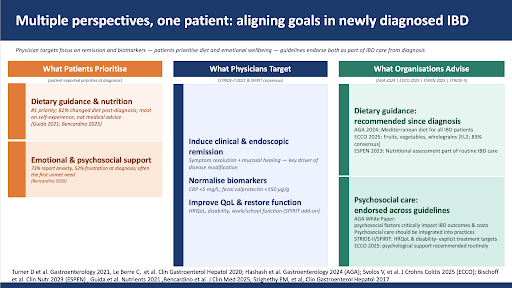
Common gaps in implementing available evidence on dietary and psychosocial support from bench to bedside include fragmented evidence, limited training among IBD providers in implementing and monitoring dietary and psychological therapies, poor patient adherence, which requires regular follow-up and coping skills, and a shortage of IBD-specialized dietitians and resilience-based care models.
Cultural Adaptation of Diet and Eating Earlier is as Important as What to Eat
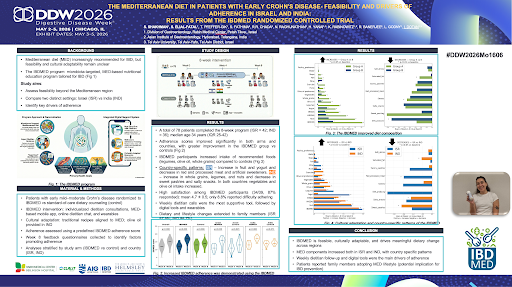
Tailoring the diet to cultural diversity, lifestyle, disease severity, and patients’ preferences may influence dietary habits, nutrition perceptions, and health outcomes. New findings from the 8-week IBDMED randomized controlled trial revealed that the Mediterranean diet is feasible, culturally adaptable, and drives meaningful dietary changes in both patients with Crohn’s disease and their family members in Israel and India. Participants increased their intake of legumes, olive oil, and whole grains compared to controls, and weekly dietitian follow-up and digital tools were the main drivers of consistency6.
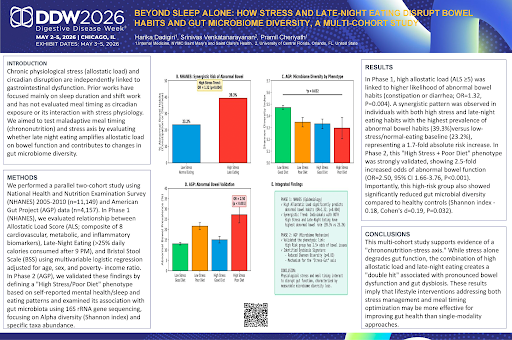
Eating earlier and avoiding late-night eating may be as important as what the patient eats. A survey from 15,306 Americans showed that people who consumed more than 25% of their daily calories after 9 p.m. and reported high stress had nearly double the odds of constipation or diarrhea and lower gut microbiome diversity compared to those who did not7. While this research was not conducted in people with GI disorders, it helps explain why some patients experience worse GI symptoms the morning after eating late or eating a lot the night before.
Diet in Crohn’s Disease and Ulcerative Colitis: What’s New?
Adding fecal microbiota transplantation to the Crohn’s Disease Exclusion Diet (CDED) improved combined clinical-endoscopic response at 52 weeks in mild-moderate CD (41.2% vs 0%), but did not achieve improvement in clinical response or remission at 12 weeks as compared to receiving CDED plus sham infusions8. Other findings revealed that a culturally adapted, microbiota-targeted Mediterranean diet program for 8 weeks was feasible and improved clinical outcomes, quality of life, and fecal calprotectin (50% reduction versus 40% in the control group) in patients with early CD from Israel and India. Clinical improvement might be mediated by an increase in gut microbiome diversity and butyrate producers9.
The Mediterranean diet promotes gut health and reduces inflammation, and can be considered in the maintenance of ulcerative colitis (UC). When it comes to dietary therapy for UC, a plant-based diet while continuing on standardized medical therapy did not significantly reduce relapse or improve quality of life, but produced favorable gut microbiome shifts, which supports further study as an adjunct10.
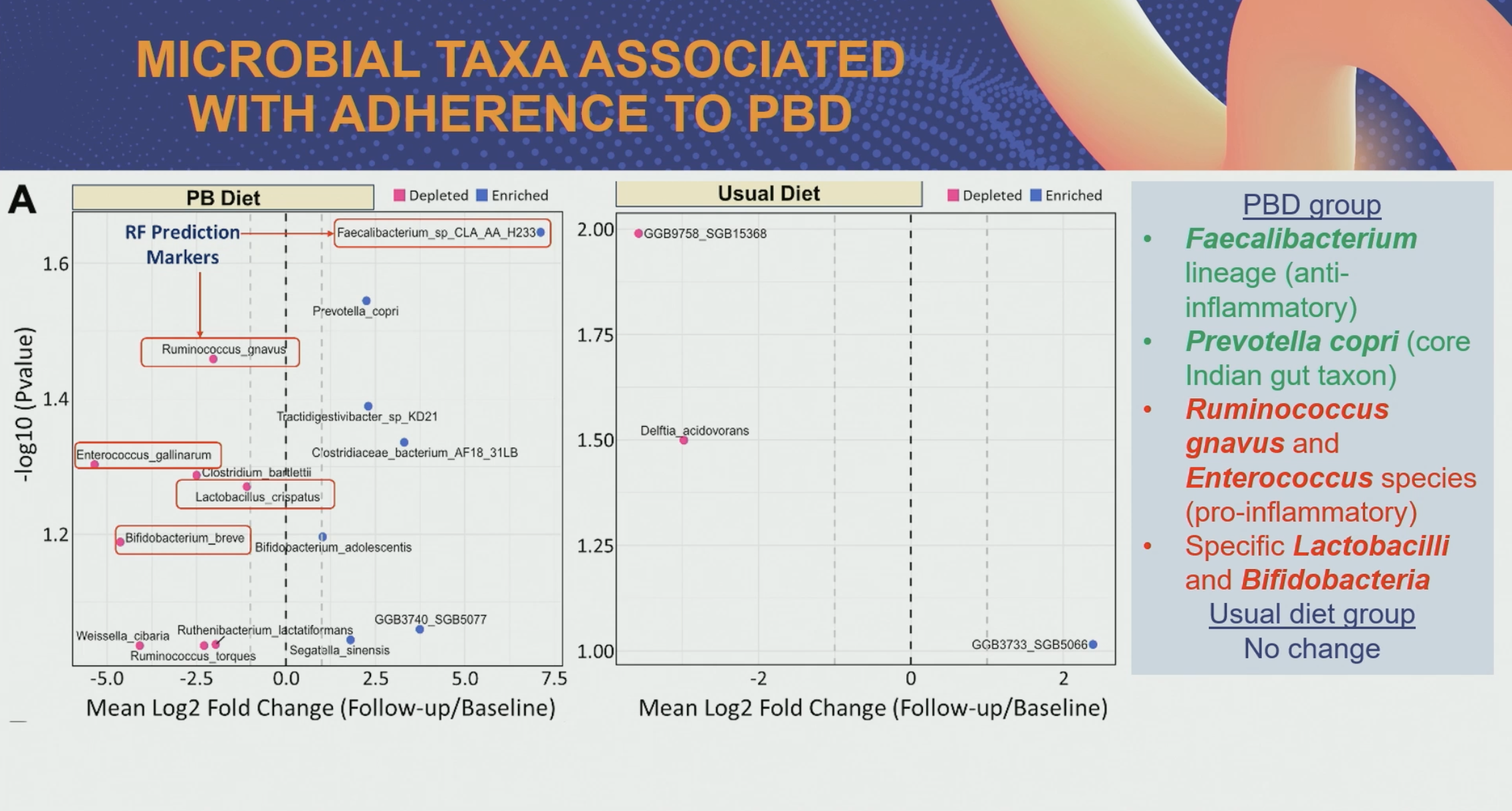
Recent findings from Natasha Haskey and colleagues at the University of British Columbia found that integrating diet, clinical data, and stool-derived markers, in particular host- and microbiota-derived metabolites, outperformed self-reported dietary intake in predicting UC disease activity. This research highlights the potential of precision nutrition-guided treatments for patients with a heterogeneous disease that responds differently to available treatments11.
Making Sense of Gluten and Gluten-Related Disorders
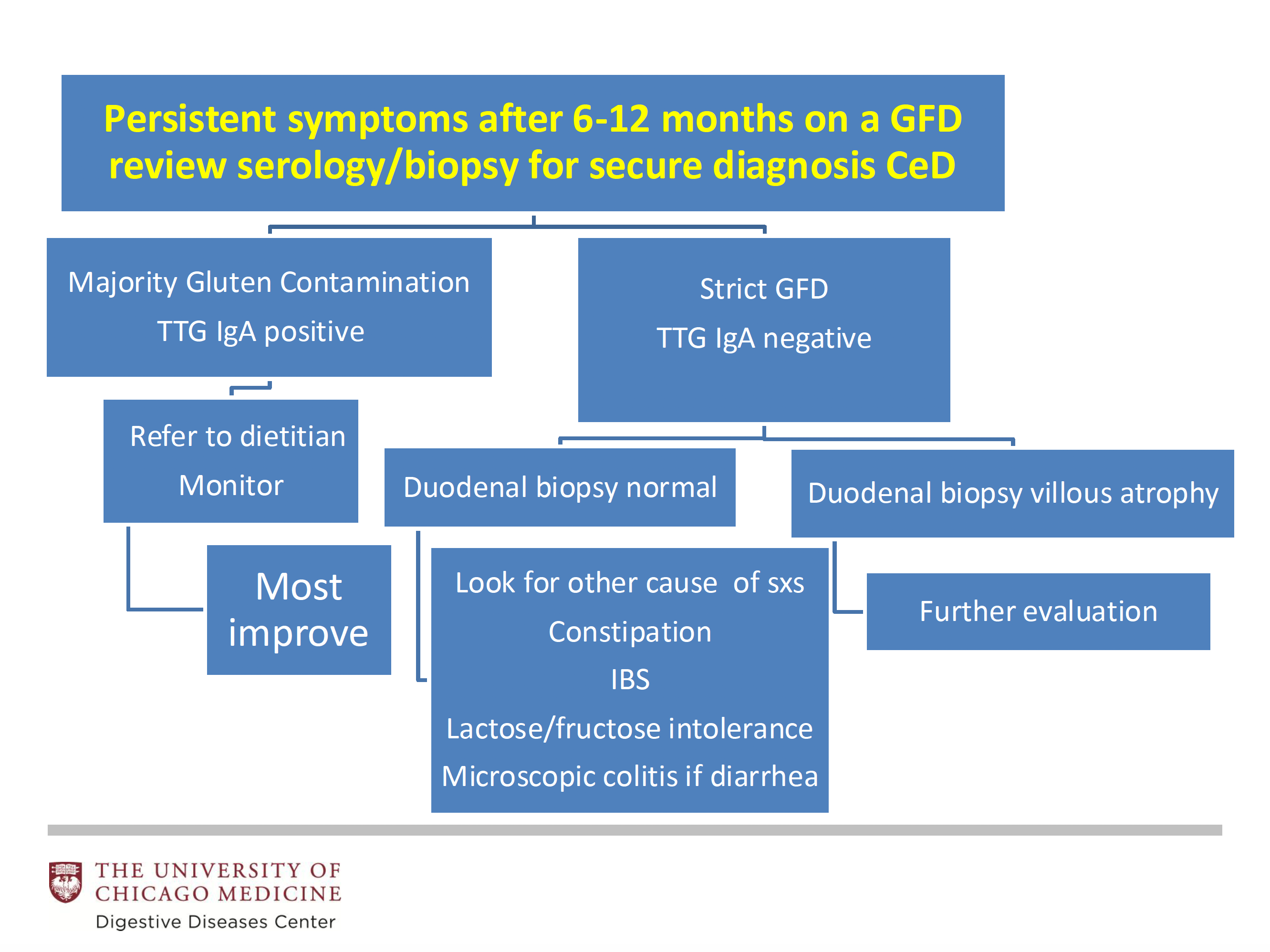
Celiac disease (CeD) is an important diagnosis to keep in the radar in a patient with digestive symptoms before labeling them as IBS. While a gluten-free diet is the only current treatment for CeD, Carol E. Semrad, MD, from the University of Chicago Medicine, acknowledged that 7-50% patients do not respond to removing gluten. The reality is that refractory CeD, defined as celiac disease with persistent villous atrophy on a gluten-free diet for a year, is rare (0.3%). Most patients do not improve due to gluten contamination. For others, it is important to consider a possible misdiagnosis and explore other causes of symptoms and enteropathies (e.g., gluten ingestion, drugs, autoimmune origin, common variable immunodeficiency, lymphoma).
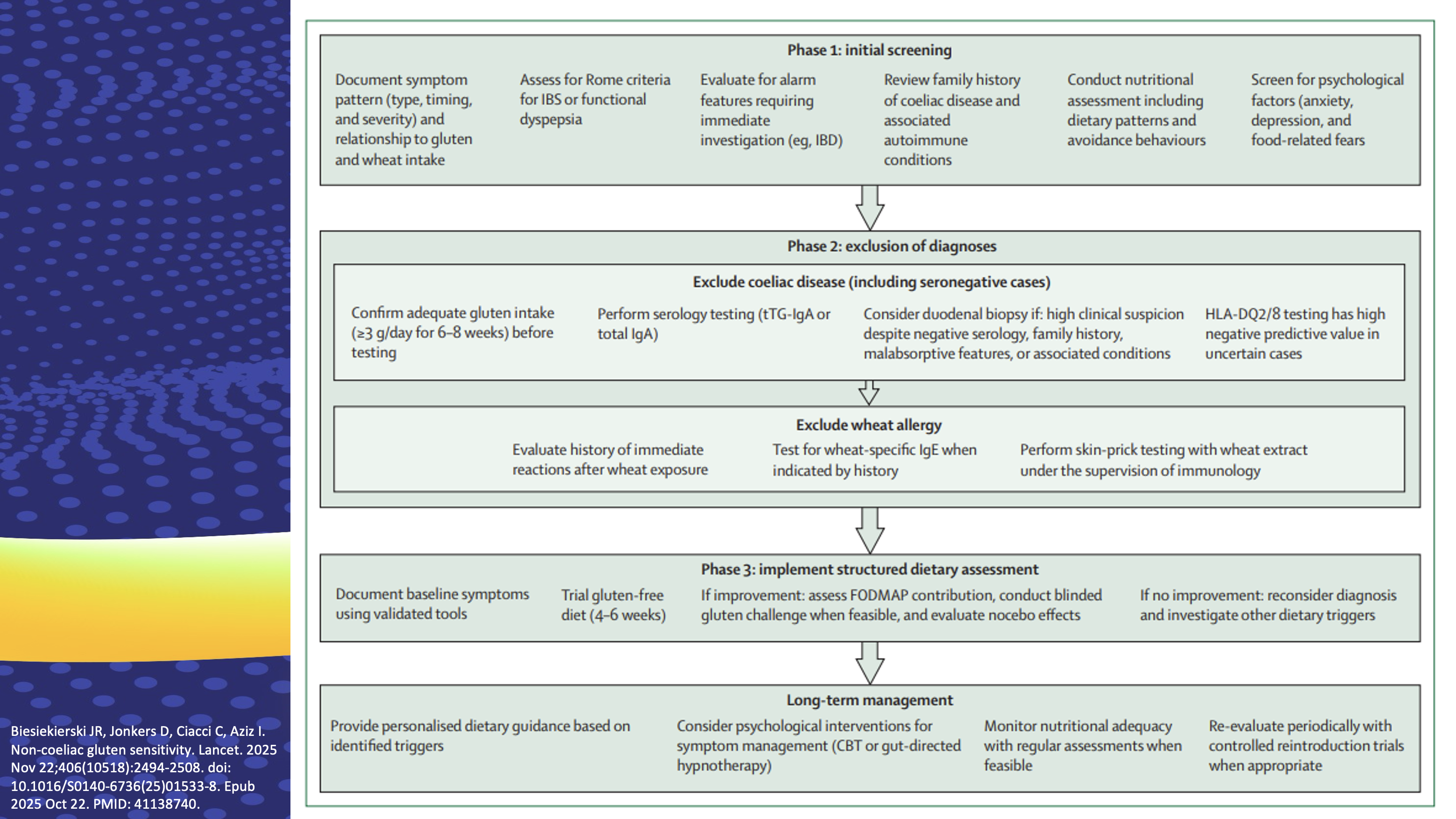
Gluten and wheat are safe to eat for many people living with IBS. While some patients with non-celiac gluten sensitivity have subtle changes in the duodenal mucosa12, recent research has revealed that fructans in wheat may be driving symptoms in most cases. Patient’s expectations and beliefs may also drive symptoms, as some people with non-celiac gluten sensitivity may experienceincreased systemic reactivity and heightened awareness ofgluten-containing foods compared to healthy controls13,14. Even with CeD, where the gluten-free diet is mandatory, if poor education or an unbalanced diet is achieved, eating disorders, psychological side effects, and deficiencies (e.g., fiber, vitamin D, vitamin B12, and folate) can occur.
Towards Less Restrictive, “Step-Up” Diets to Improve the Quality of Life of Patients with Eosinophilic Esophagitis
The number of cases of eosinophilic esophagitis (EoE) is increasing, regardless of location. Exposures in the antenatal and perinatal periods and in the first year of life may increase the risk of EoE. Evan S. Dellon, MD, MPH, from the University of North Carolina School of Medicine, highlighted that maternal infection or fever, antibiotics in the first year of life, Cesarean delivery, neonatal intensive care unit stay, and acid suppressant use in the first year of life have been shown to increase risk of development of EoE in both children and adults15.
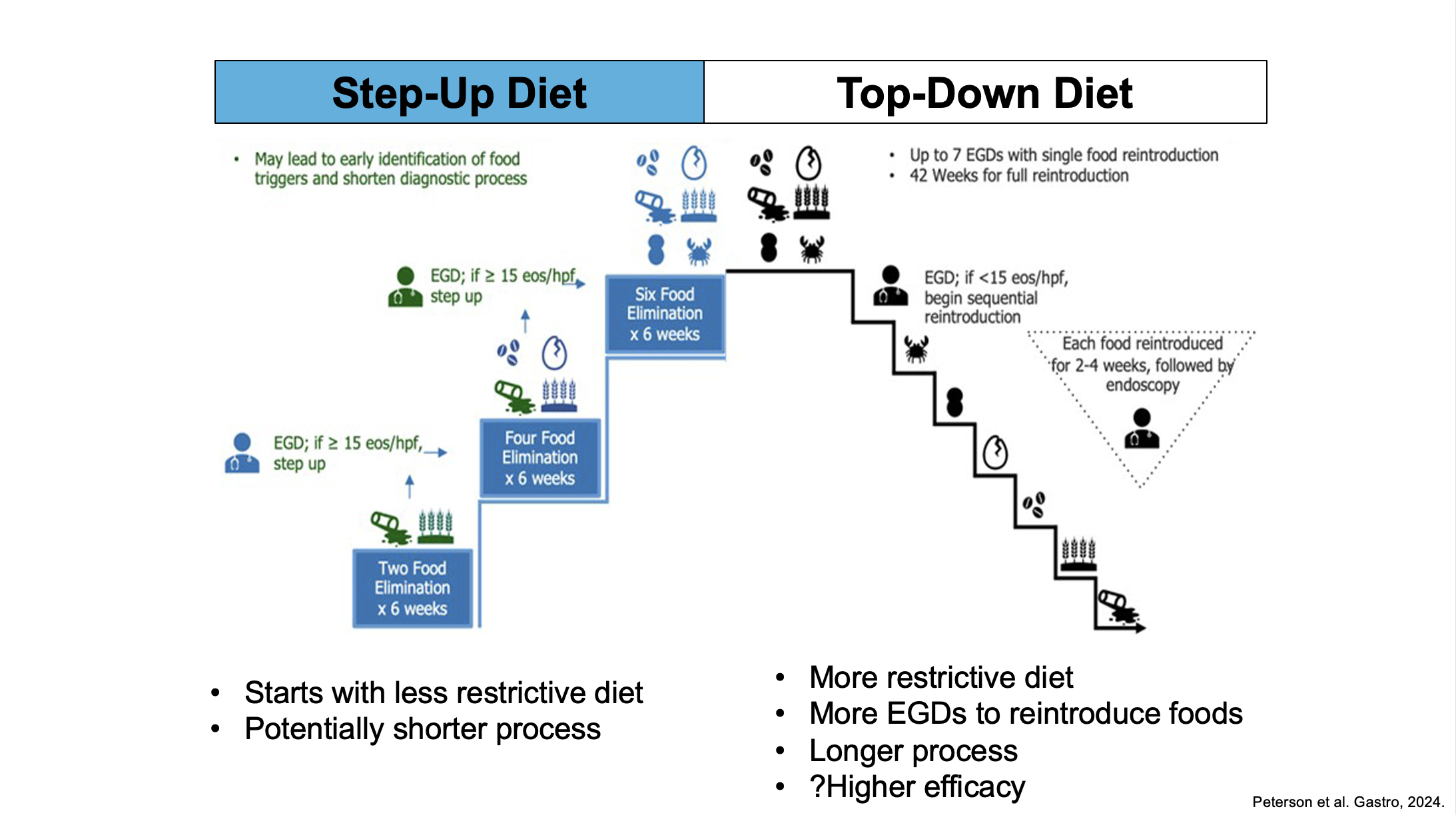
Joy W. Chang, MD, MS, from the University of Michigan, delved into which diet to choose for patients with EoE who elect it and how to do it efficiently. The latest American College of Gastroenterology guidelines suggest shared decision-making should play a role in determining the first-line treatment (pharmacologic or diet elimination treatment) with consideration of the severity of EoE16. While initial studies focused mainly on the 6-food elimination diet, two recent randomized trials produced data in support of less-restrictive diets that may balance quality of life and efficacy:
- The multicenter 6-Food versus 1-Food Eosinophilic Esophagitis Elimination Diet (SOFEED) randomized trial in adults with active EoE (n=129) showed histological, endoscopic, quality of life, and molecular changes in the EoE transcriptome improvements were similar in the group who followed a 1-food elimination diet (1FED [dairy]) and the group who followed a 6-food elimination diet (dairy, wheat, egg, soy, nuts, and seafood) for 6 weeks (23 (34%) of 67 patients on the 1FED and 25 (40%) of 62 patients on the 6FED at 6 weeks). The 4FED withdrawal rate (32%) exceeded that of 1FED (11%)17.
- In the second randomized trial, a total of 63 patients < 18 years with active EoE nonresponsive to proton pump inhibitor therapy were randomized to the 1-food elimination diet (1FED [dairy]) versus a 4-food elimination diet (4FED [dairy, wheat, egg, and soy]) for 12 weeks (phase I). The 1FED nonresponders were assigned to treatment with a 4FED, whereas the 4FED nonresponders were assigned to treatment with swallowed glucocorticoids for 12 additional weeks (phase II). Endoscopic, histologic, and molecular changes (transcriptome) findings were similar across treatment arms. Indeed, the rate of histologic remission was 44% for the 1FED versus 41% for the 4FED. Withdrawal rates were higher for the 4FED (32%) than for the 1FED (10.5%) at 12 weeks18.
Given the complexity of avoiding six foods and the great difficulty of sustaining such an effort for more than a year, this evidence favors the relative simplicity and feasibility of dairy elimination as an initial approach to the dietary management of EoE. Chang also shared a practical guide to implement and monitor diet therapy for EoE, which is particularly useful in the context when the patient does not have access to a registered dietitian.
Targeting the Microbiome for GI Disorders: Hype or Hope?
Patients with IBS come to the clinic with positive microbial stool testing or altered breath test for intestinal methanogen overgrowth and ask what to do. Eamonn M. Quigley, MD, PhD, chief of Gastroenterology at the Houston Methodist Hospital, explained that available commercial direct-to-consumer microbiome tests are not standardized or validated and are only informative of fecal microbiota but not microbiota in the small bowel or in close contact with gut mucosa. Some key processes of the gut microbiome occur at the strain and microbial-derived metabolites levels, which are not always tracked. We do not yet know what a normal or healthy gut microbiome is, so direct-to-consumer microbiome tests are not informative about the best diet or probiotic to take19.
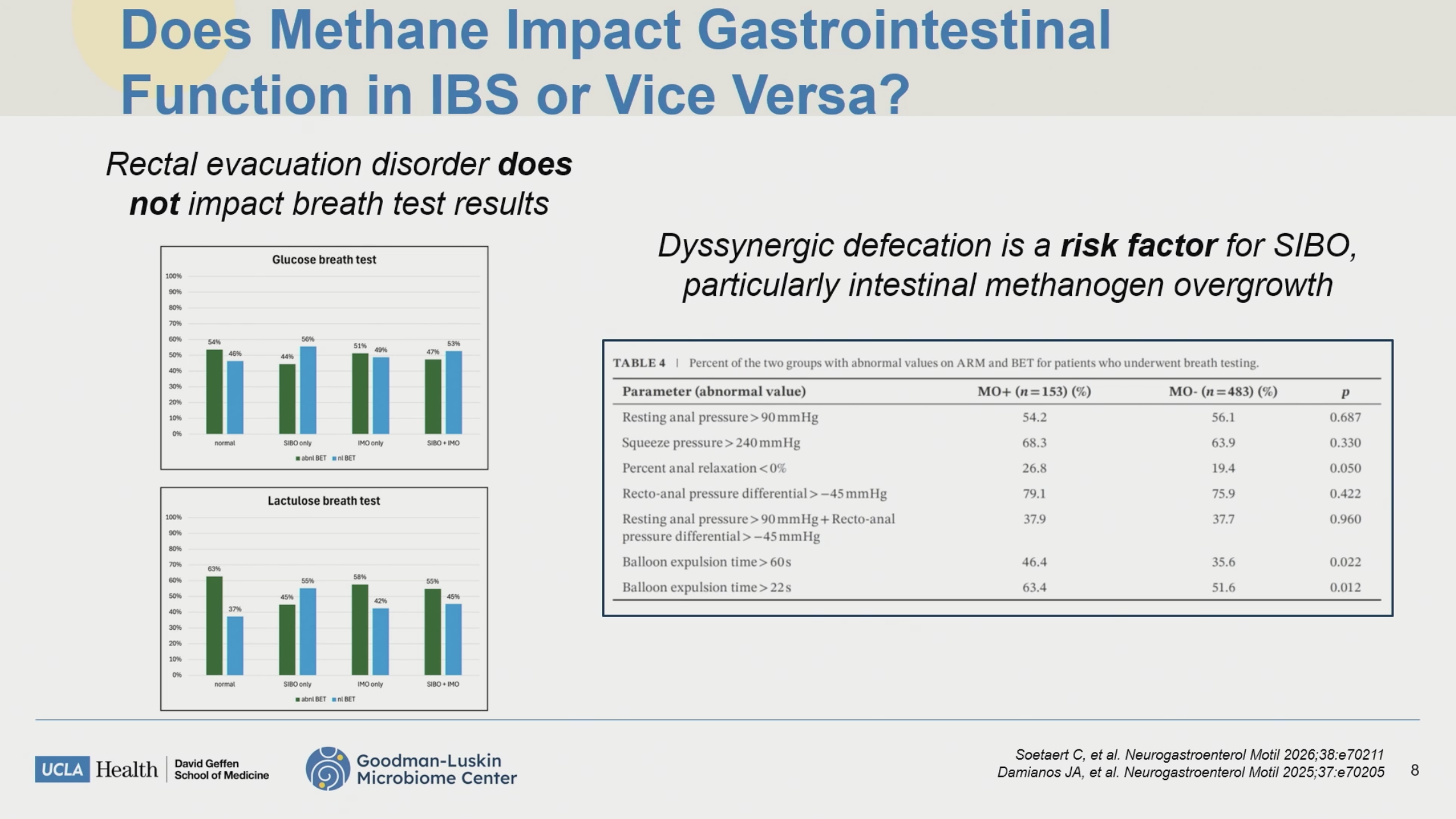
Andrea S. Shin, MD, MSc, University of California Los Angeles, acknowledged that the cause or effect of methane in IBS is not yet established, the increase in methane may arise from overgrowth of methanogens in the colon, and host-specific factors (e.g., transit time), diet, medications, and compliance to test protocols can affect diagnostic accuracy. When it comes to the management of intestinal methanogen overgrowth, there is limited evidence for combination of antibiotic protocols and the treatment should be individualized to acknowledge biological plausibility (i.e., a causal relationship between a microbe and symptoms) and the clinic of the patient.
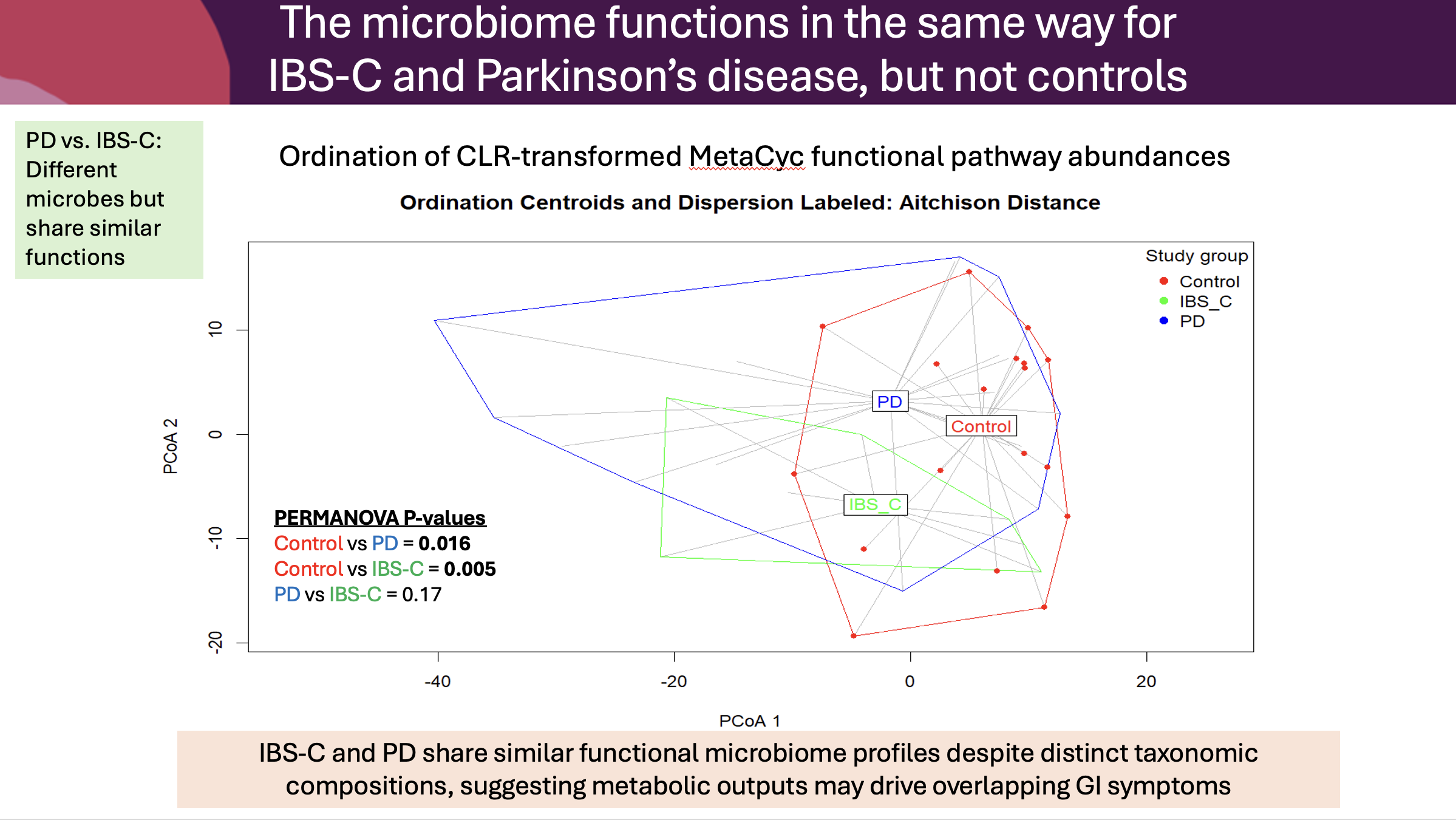
Regarding new evidence on microbiome-targeted interventions, a 4-week probiotic intervention (Bifidobacterium quadruple viable tablet) significantly reduced spontaneous neural activity in the right insula (involved in the awareness of internal bodily sensations and the emotional perception of pain. The probiotic upregulated functional pathways and circulating metabolites related to GABA synthesis and metabolism, particularly ornithine. These findings suggest a potential gut–brain axis mechanism whereby probiotics may exert therapeutic effects in IBS through modulating metabolism and central excitatory–inhibitory balance20. Nicholas Talley, MD, PhD, at the University of Newcastle (Australia), provided new evidence to support a complex interplay between gut microbiome composition, microbial functional capacity, and immune activation in Parkinson’s disease, with partial constipation overlap. These findings highlight that while constipation is a shared symptom, the underlying mechanisms differ substantially between these conditions, with PD showing unique signatures in immune reactivity and microbial metabolic pathways relevant to neurotransmission and vitamin biosynthesis21.
On the other hand, up to 50% of patients with an ileal pouch-anal anastomosis develop pouchitis and the gut microbiome may be involved given high antibiotic exposure. A randomized controlled trial showed weekly FMT for 6 weeks did not improve remission over placebo in antibiotic-dependent or refractory pouchitis22. In contrast, FMT improved endoscopic response over placebo in active CD with a profound donor-potency effect. The authors acknowledged that the non-significant Crohn’s disease activity index (CDAI) result may reflect the strong pre-randomization diet and antibiotic ruin-in23.
Digestive Disease Week 2027 is scheduled for 15-18 May in Washington DC, USA.
References:
- Grover M, Barbara G, Chey W, et al. The intestinal microenvironment and disorders of gut-brain interaction. Gastroenterology. 2026; 170(6):1133-1151. doi: 10.1053/j.gastro.2026.02.015.
- Wang XJ, Nguyen LAB. “Functional” GI conditions in the older adult: DGBIs and beyond. Am J Gastroenterol. 2025; 120(Suppl 10):S45-S55. doi: 10.14309/ajg.0000000000003641.06.
- Moran GW, Leslie FC, McLaughlin JT. Crohn’s disease affecting the small bowel is associated with reduced appetite and elevated levels of circulating gut peptides. Clin Nutr. 2013 Jun;32(3):404-11. doi: 10.1016/j.clnu.2012.08.024.
- Lacy BE, Cangemi D, Vazquez-Roque M. Management of chronic abdominal distension and bloating. Clin Gastroenterol Hepatol. 2021; 19(2):219-231.e1. doi: 10.1016/j.cgh.2020.03.056.
- Koloski N, Jones M, Shah A, et al. Irritable bowel syndrome is associated with a 2.5 fold increased risk of infertility among primary care patients [Guided Poster Session, Su1764] Digestive Disease Week® (DDW) 2026, Chicago.
- Shakhman S, Elial-Fatal S, Pfeffer-Gik P, et al. (2026, May 2-5). The Mediterranean diet in patients with early Crohn’s disease - feasibility and drivers of adherence in Israel and India: results from the IBDMED randomized controlled trial [Guided Poster Session, Mo1606] Digestive Disease Week® (DDW) 2026, Chicago.
- Dadigiri H, Venkatanarayanan S, Cheriyath P, et al. (2026, May 2-5). Beyond sleep alone: how stress and late-night eating disrupt bowel habits and gut microbiome diversity, a multi-cohort study [Guided Poster Session, Mo1769] Digestive Disease Week® (DDW) 2026, Chicago.
- Arora U, Madam D, Raval NP, et al. FMT plus exclusion diet in Crohn’s disease. A 52-week randomized, double-blind, sham-controlled trial. Presented at DDW 2026. Trial CTRI/2022/10/046861.
- Godny L, Raghunathan N, Reshef L, et al. The Mediterranean diet improves clinical and inflammatory outcomes in patients with early Crohn’s disease: results from the IBDMED randomized controlled trial. Presented at DDW 2026. Trial NCT05536544.
- Narang H, Madan D, Shete O, et al. Plant-based diet for maintaining remission in ulcerative colitis: 12-month randomized controlled trial. Presented at DDW 2026. Trial CTRI/2022/02/04/041032.
- Haskey N, Morton J, Sanders J, et al. (2026, May 2-5). Predicting clinical response to the Mediterranean diet through stool-omic signatures in ulcerative colitis: an exploratory study [Guided Poster Session, Sa1761] Digestive Disease Week® (DDW) 2026, Chicago.
- Rostami K, Ensari A, Marsh MN, et al. Gluten induces subtle histological changes in duodenal mucosa of patients with non-coeliac gluten sensitivity: a multicentre study. Nutrients. 2022;14(12):2487. doi: 10.3390/nu14122487.
- Iven J, Geeraerts A, Vanuytsel T, et al. Impact of acute and sub-acute gluten exposure on gastrointestinal symptoms and psychological responses in non-coeliac gluten sensitivity: a randomised crossover study. United European Gastroenterol J. 2025 Sep;13(7):1295-1306. doi: 10.1002/ueg2.70014.
- Biesiekierski JR, Jonkers D, Ciacci C, et al. Non-coeliac gluten sensitivity. Lancet. 2025; 406(10518):2494-2508. doi: 10.1016/S0140-6736(25)01533-8.
- Visaggi P, Dellon ES. Epidemiology, natural history, and treatment of eosinophilic gastrointestinal diseases. Gastroenterology. 2026;170(3):476-494. doi: 10.1053/j.gastro.2025.09.030.
- Dellon ES. Guidelines in practice: diagnosis and management of eosinophilic esophagitis. Am J Gastroenterol. 2025; 120(10):2223-2225. doi: 10.14309/ajg.0000000000003386.
- Kliewer KL, Gonsalves N, Dellon ES, et al. One-food versus six-food elimination diet therapy for the treatment of eosinophilic oesophagitis: a multicentre, randomised, open-label trial. Lancet Gastroenterol Hepatol. 2023; 8(5):408-421. doi: 10.1016/S2468-1253(23)00012-2.
- Kliewer KL, Abonia JP, Aceves SS, et al. One-food versus 4-food elimination diet for pediatric eosinophilic esophagitis: A multisite randomized trial. J Allergy Clin Immunol. 2025; 155(2):520-532. doi: 10.1016/j.jaci.2024.08.023.
- Porcari S, Mullish BH, Asnicar F, et al. International consensus statement on microbiome testing in clinical practice. Lancet Gastroenterol Hepatol. 2025; 10(2):154-167. doi: 10.1016/S2468-1253(24)00311-X.
- Liu X, Zhang K, Xu Z, et al. Neuroimaging modulatory effects of probiotics in IBS: a single-center, randomized, double-blind, placebo-controlled clinical trial. Presented at DDW 2026.
- Hoedt EC, Burns GL, Hedley KE, et al. Shared functional microbiome signatures in Parkinson’s disease and constipation predominate irritable bowel syndrome despite taxonomic divergence. Brain Behav Immun Health. 2026; :53:101218. doi: 10.1016/j.bbih.2026.101218.
- Syed SA, Delungahawatta T, Patel J, et al. Fecal microbiota transplantation for the induction of remission in active pouchitis: a randomized controlled trial. Presented at DDW 2026.
- Fehily SR, Wright EK, Bogatic D, et al. Faecal microbiota transplantation for active Crohn’s disease: the MIRO (Microbial Restoration) randomised placebo-controlled trial. Presented at DDW 2026.




Support our Mission
Your donation will help us to enhance the well-being and health outcomes of patients with GI conditions.
Donate